Vol. X: Debunking Vaporizer Myths
Explore expert Q&A on WAG systems, safety, and best practices in veterinary anesthesia. Learn more…

This issue of Vapors will review the concept of dead space and more specifically mechanical dead space. It is necessary to first define the general term dead space or “dead volume”. It is that portion of the tidal volume that does not contribute to alveolar ventilation. For example, the gas remaining in the trachea at the end of expiration is “dead volume”. It has had oxygen removed and carbon dioxide added in the alveoli, therefore during the next inspiration that “dead volume” of gas is moved into the alveoli but will not provide oxygen. This is also “dead volume” during expiration because the gas in the trachea is not removing carbon dioxide from the lungs. The upper airway, trachea, and bronchioles are all considered “dead volume” and are defined as anatomical dead space. This “dead volume” comprises approximately 30% of a normal resting tidal volume. As a matter of observation the anatomical dead space is actually reduced when an endotracheal tube is inserted because the tube must be smaller than the trachea.
The issue of mechanical dead space is the focus of this discussion and is defined as any volume that is added by any equipment attached to the endotracheal tube. This includes airway monitors, connector elbows, the breathing tube Y piece, and also includes any portion of the endotracheal tube that extends beyond the mouth. As one observes the patient connected to the equipment, the mechanical “dead volume” is any volume that moves back and forth instead of in only one direction as the patient breathes. Therefore any gas that moves toward the patient during inspiration and away from the patient during expiration is not “dead volume” but is contributing to alveolar ventilation.
So what? Is this really important to anesthesia? How does too much mechanical “dead volume” affect anesthesia? Or does it? It should be obvious from the definitions above that if too much of the tidal volume is “dead volume” carbon dioxide levels will increase and inspired concentrations of oxygen and anesthetic will decrease. If the patient is on 100% oxygen the decrease in oxygen is probably not significant but carbon dioxide and anesthetic concentrations will be affected. If the anesthetic concentration is decreased this can lead to a plane of anesthesia that is too light and increased carbon dioxide will lead to an increased respiratory rate and a respiratory acidosis.
There is sometimes a misconception that the breathing tubes are “dead volume”. This seems to the casual observer to be true, but in reality the gas only moves toward the patient through the inspiratory tube and away from the patient through the expiratory tube. The question is – what causes the gas to move one way through the tubes?
In fact, it is one of the most important components of the anesthetic machine – the one way valve discs. When the discs function properly there is very little dead space in the breathing tubes. However, if the discs are not functioning properly, the anesthesia procedure can be difficult.
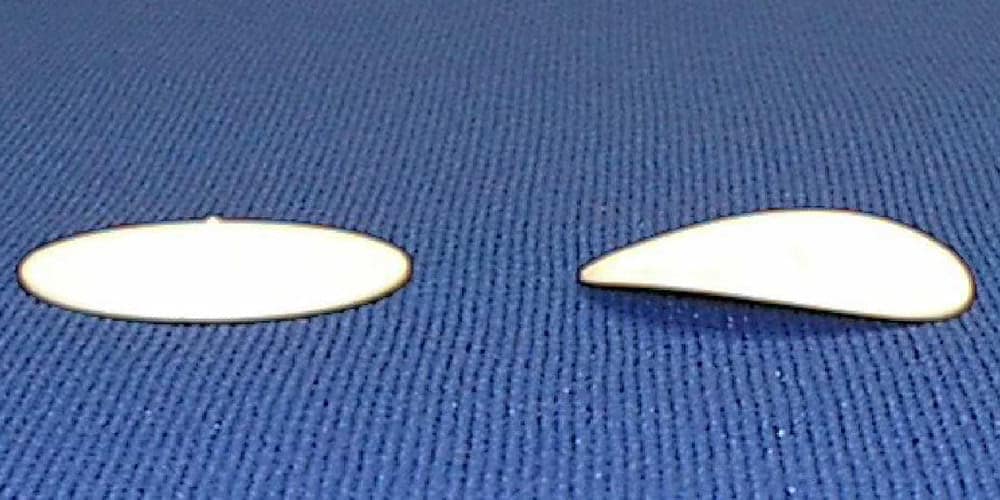
The discs must be flat so there is a tight seal on the surface of the one way valve body to function properly. When the one way valve disc is lifted from the surface of the valve it is open and allows gas through the valve. When it lays flat on the valve surface it is closed. Casual observation of the movement of the discs as the patient breathes will indicate they are functioning but may not be sealing. Failure to seal is usually a result of the one way disc being warped (see fig. 1). This usually happens in machines that are older but occasionally is found in newer machines. The discs can be checked by removing and placing them on a flat table or counter top (see fig 2).
Failure to seal can also be a result of dirt on the disc or valve surface. Sometimes the valve surface becomes corroded and needs to be cleaned to allow a proper seal. Soda sorb dust can also accumulate on both the disc and valve causing a failure to seal.
There is not a quantitative answer to this question, however when an increase of inspired carbon dioxide is reported to a Vetamac technician it is usually a one way valve problem. If capnography is not used it is more difficult to isolate the problem until it becomes severe enough to create difficult anesthesia. Increased mechanical dead space due to one way valve disc failure should be a consideration when attempting to isolate problems with anesthesia.