
Did You Know Your Oxygen Costs? Discover How Much You Could Save!
Discover how much you could save on oxygen costs with our insightful guide. Uncover potential…
Concerning the use of intermittent positive pressure ventilation (IPPV) with the use of a mechanical means three keys points need to be considered. They are:
The number one key point to using the ventilator is to make sure the anesthesia machine does not leak. If the machine leaks, then the ventilator will leak and not function properly.
Once a proper leak test has been performed on the anesthesia machine (as described in Vapors Vol. VII, Issue 3 Fall 2016), the ventilator can be connected to the anesthesia machine and the bellows, housing & hoses can be tested for leaks.
Common leaks with the ventilator are:
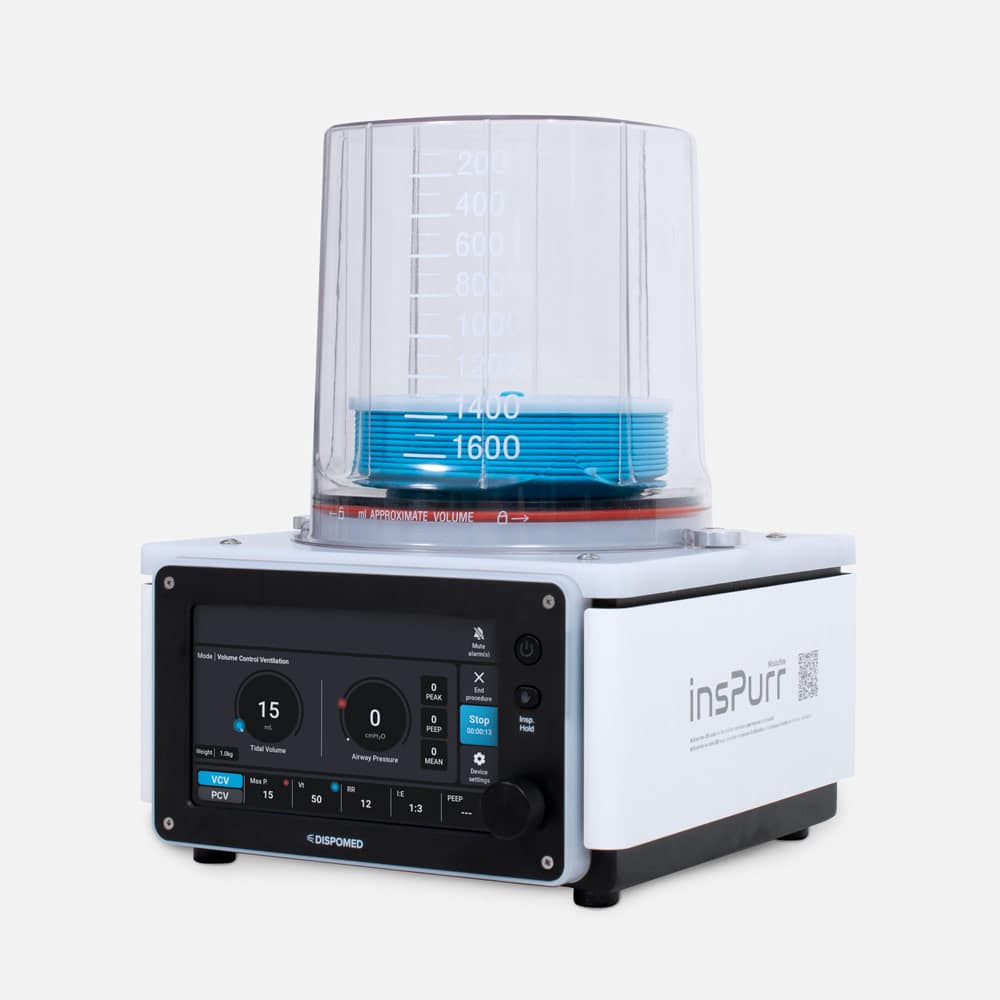
There are two types of bellows which are more recently described as Standing (ascending) or Hanging (descending). The description of Standing or Hanging describe the position of the bellows during the expiratory pause. The majority of modern ventilators use the Standing bellows which can be easily checked for leaks. Remove the reservoir bag from the anesthesia machine and replace it with the output tubing on the ventilator. Fill the bellows with either the flowmeter or flush valve. Never use the flush valve when a patient is connected to the ventilator. Once the bellows reach the top of the housing, turn off the flow of oxygen and observe the bellows. They should remain at the top of the housing and not fall if the system is free of leaks.
Now that the equipment is ready for use the next key point to consider is when should IPPV be used. There are several factors to consider when answering this question. Some of the factors to consider are respiratory rate, EtC02, tidal volume, positioning, length of the procedure and cardiopulmonary disease. There are also certain situations where ventilating the patient is necessary. Examples are thoracotomies, diaphragmatic hernias, apnea and hypercapnia. Consideration should also be given to the fact that the use of IPPV will inevitably reduce blood pressure and cardiac output in all species. This is due to during inspiration positive pressure replaces the negative pressures that develop during spontaneous respiration. This will restrict the venous return and cause blood pressure to decrease. Therefore, it is recommended to measure blood pressure either by non-invasive or invasive means prior to initiating IPPV. It is much easier to correct hypotension and then initiate IPPV than to ventilate immediately and try to correct the hypotension.
Hypercapnia is another factor to consider when ventilating a patient. There is controversy about when to ventilate based on the numbers received from capnography. Normal arterial CO2 (Pa CO2) is 35-45mmHg in all species. The number received from a capnometer is EtC02 and is typically 5-1 OmmHg lower than PaC02. (Ex: EtC02 of 50 mm Hg will be a PaC02 of 55 – 60 mmHg). The controversy lies in how high to allow EtC02 before ventilating a patient. Studies have shown benefits to a mild hypercapnia (EtC02 50 – 55 mm Hg) known as permissive hypercapnia. By not ventilating these patients the blood pressure and cardiac output may actually improve. Therefore, it is important to treat every patient individually and evaluate all the parameters.
Equine: 1200 lb. mare in dorsal recumbency for an ovarian tumor. Arterial catheter is placed, and hypotension is corrected with a CRI of Dobutamine. Respiratory rate is 5 bpm and EtC02 is 55 mmHg and the length of the surgery is estimated at one hour. Prolonged periods of hypercapnia can lead to myocardial depression and respiratory acidosis. Initiating IPPV at the beginning of this case would prevent these complications. IPPV will also assist in reaching a plane of surgical anesthesia quicker than spontaneous ventilation.
Canine: 80 lb. Spinone in dorsal recumbency for ruptured cruciate repair. Premedication of opioids and acepromazine and induction with Propofol. Respiratory rate (RR) of 8 bpm, EtC02 is 45 mm Hg and systolic blood pressure (SBP) is 100 mm Hg. Surgery time is estimated at 40 minutes. Upon surgical stimulation the patient awakes, RR increases, SBP increases more Propofol is given and the inhalant is increased to 3%. Patient’s SBP reduces to 80 mm Hg, RR rate is 6 bpm and the inhalant is decreased to 1.5%. Ten minutes later the patient awakens, and the same scenario is repeated. Placing this patient on a ventilator once the SBP is > 90 mm Hg will stop the “roller coaster” effect of this case and allow the reduction of inhalant and help maintain a surgical plane of anesthesia.
It is impossible to address all the specifics in this article for when to ventilate your patients. Please realize these are only guidelines and the specific settings should be determined by the individual patients and their specific needs.
| Respiratory Rate (RR) | Peak Inspiratory Pressure (PIP) | Tidal Volume (TV) | |
|---|---|---|---|
| Equine | RR: 6-10 bpm | PIP: 20-30 cm H20 | TV: 1U100 kg (10 ml/kg) |
| Swine | RR: 8-18 bpm | PIP: 15-20 cm H20 | TV: 10-15 ml/kg |
| Ruminants | RR: 8-12 bpm | PIP: 15-25 cm H20 | TV: 13-18 ml/kg |
| Canine | RR: 8-12 bpm | PIP: 10-20 cm H20 | TV: 10-15 ml/kg |
| Feline | RR: 10-14 bpm | PIP: 10-20 cm H20 | TV: 10-15 ml/kg |


Veterinary Specialist Articles