

Did You Know Your Oxygen Costs? Discover How Much You Could Save!
Discover how much you could save on oxygen costs with our insightful guide. Uncover potential…

Veterinary anesthesia patients greatly benefit from using an automated alternative to the reservoir bag in their breathing systems. This innovation not only enhances respiratory regulation but also ensures a more consistent depth of anesthesia for small animals. Pet owners expect the best care for their furry companions, and it is our responsibility to meet those expectations. With improved products and more affordable educational resources, many small animal clinics are transitioning to provide a safer anesthesia experience.
A mechanical Ventilator is a machine that generates a controlled flow of gas into a patient’s airways.
Intermittent positive pressure ventilation is applied solely during inspiration, whether manually or mechanically.
Positive End-Expiratory Pressure (PEEP) is utilized to keep small airways open during the expiration phase, helping to prevent atelectasis and manage conditions such as chronic airway disease, lung trauma, or pulmonary edema. Typical PEEP levels range from 1 to 7.5 cm H2O.
Peak Inspiratory Pressure (PIP) refers to the pressure in the airway during inhalation, typically set between 12 and 20 cm H2O.
Tidal Volume is the total volume of air inhaled and exhaled in a single breath, typically calculated at 10-20 mL/kg and measured using respirometry.
Minute Ventilation is calculated by multiplying tidal volume by the respiratory rate (RR). For example, a tidal volume of 200 mL multiplied by a respiratory rate of 10 results in a minute ventilation of 2 liters.
Breath cycle measurement involves assessing both the inspiratory and expiratory phases. The duration of each phase is determined by the ratio of inspiration to expiration, along with the overall respiratory rate.
Inspiratory Time refers to the duration required to inflate the lungs, typically around 1 second for small animal patients.
The number of cycles per minute is known as the respiratory rate during spontaneous breathing.
Partial pressure of oxygen (PaO2) refers to the amount of oxygen dissolved in arterial blood.
Partial pressure of carbon dioxide (PaCO2) indicates the concentration of carbon dioxide dissolved in arterial blood.
End-Tidal Carbon Dioxide (ETCO2) is the measurement of carbon dioxide in the alveoli, sampled near the endotracheal tube. It closely correlates with the patient’s arterial CO2 levels, which typically range from 35 to 45 mmHg.
Quantitative measurement of respiration refers to the assessment of respiratory function.
Alongside tissue perfusion and blood pressure support, maintaining a clear airway is crucial for patients undergoing anesthesia. When a patient is sedated, premedicated, or anesthetized, their respiratory efforts often diminish, resulting in a reduced breathing rate and less pronounced chest movements. This impairment hampers the patient’s ability to exchange gases effectively (oxygen for carbon dioxide).
Decreased respiratory efforts in a sedated patient can lead to hypoxemia, which is often a result of hypoventilation (increased carbon dioxide levels). Preoxygenation is vital during the pre-operative phase, and continued oxygen support is necessary in the recovery period until normal ventilation is restored (with ETCO2 levels between 35-45 mm Hg and SpO2 greater than 95%).
Following induction and intubation, airway support must be maintained. Regular ventilation assistance becomes essential if one or more of the following issues arise:
Both manual and mechanical ventilation play critical roles in veterinary anesthesia, especially for patients with pre-existing conditions or those who develop complications requiring alveolar gas exchange support. Many veterinary practices already implement manual breaths to assist in ventilation, which is essential for patients who become apneic or exhibit shallow breathing. However, this approach necessitates that a dedicated team member pause their duties to provide necessary airway support.
With advancements in education and technology, an increasing number of veterinary practices are adopting mechanical ventilation for their anesthesia patients. This is particularly beneficial for cases involving prolonged anesthesia or for patients with specific needs, such as obesity, deep-chested large breed dogs, and brachycephalic breeds.
Mechanical ventilators offer the advantage of controlling airway pressure, volume, and respiratory rate, all while being monitored by both the user and advanced multiparameter tools like capnography and pulse oximetry. Utilizing a mechanical ventilator allows the anesthetist to focus more on monitoring the patient effectively, enhancing overall care during procedures.


Dental procedures in veterinary medicine often involve extended periods of anesthesia, sometimes lasting several hours. During these lengthy procedures, dedicated monitoring is crucial for patient safety. One common issue that arises is pulmonary atelectasis, or the collapse of alveoli, which can begin shortly after anesthesia induction and worsen over time.
Mechanical ventilators play a vital role in reversing this process through intermittent positive pressure ventilation. Many patients undergoing extensive dental work may also receive analgesia infusions or exhibit irregular breathing patterns. By employing a balanced approach to anesthesia and analgesia alongside a mechanical ventilator, veterinary professionals can maintain a stable and smooth plane of anesthesia, ensuring optimal outcomes for their patients.
Dental patients are often positioned with their heads lower than their bodies, which can lead to increased abdominal pressure on the lungs and greater breathing resistance. Many of these patients are seniors with underlying comorbidities, and some may be brachycephalic or deep-chested. Utilizing a mechanical ventilator in these cases helps alleviate the stress associated with inadequate oxygen and carbon dioxide exchange, ensuring better respiratory function during procedures.
Most anesthesia ventilators have volume or pressure control options.
VOLUME option delivers a preset tidal volume over a specified inspiratory time. In this mode, the peak inspiratory pressure (PIP) generated is influenced by the set tidal volume, as determined by the operator, and the compliance of the respiratory system. This approach ensures consistent air delivery to the patient during ventilation.
PRESSURE limiting machines maintain a preset airway pressure during a specified inspiratory time. In this mode, the tidal volume delivered depends on the preset airway pressure set by the operator and the compliance of the respiratory system. This allows for better management of airway pressures, particularly in patients with variable lung compliance.
Veterinary professionals must have a comprehensive understanding of how anesthesia machines operate and be familiar with what constitutes “normal” vital signs in patients—such as heart rate, blood pressure, oxygen saturation, respiratory rate, and the characteristics of a normal breath, including end-tidal carbon dioxide levels. These parameters can be significantly altered during general anesthesia and mechanical ventilation. It’s essential to include a pressure alarm for monitoring safe airway pressures. Here are some guidelines to consider for optimal ventilation strategies:
Since the exchange of carbon dioxide and oxygen in the patient is controlled by the user during both manual and mechanical ventilation, it is crucial to monitor and maintain normal values using capnography, pulse oximetry, and hands-on assessment. Carbon dioxide removal is primarily achieved through minute volume. The peak inspiratory pressure (PIP) should ideally be maintained in the 15-20 cm H2O range. Whether opting for a high ventilation rate with a low tidal volume or a lower rate with a high volume, the effects will remain similar.
For time or volume-cycled ventilators, start by calculating the tidal volume. Observe the patient’s thoracic cavity to ensure bilateral chest expansion while maintaining a PIP within the recommended 15-20 cm H2O pressure range. In pressure-cycled ventilators, set the inspiratory pressure and adjust based on observed chest expansion. Additionally, monitor blood pressure, as increased thoracic expansion may reduce venous return, potentially affecting mean arterial pressures. The inspiratory time should always be shorter than the expiratory time, allowing for full thoracic expansion and effective gas exchange within the alveoli, as well as adequate time for lung recoiling.
Some mechanical ventilators are equipped with internal respirometry to measure each patient’s ventilation needs, providing a wider safety margin. When weaning a patient off the mechanical ventilator, allow the patient to accumulate carbon dioxide to trigger normal ventilation, as this is regulated by the brain’s respiratory center. You may decrease the rate and volume or continue manual ventilation support until the patient resumes normal breathing patterns. Always monitor carbon dioxide levels until the patient is regaining consciousness, along with blood oxygen saturation using a pulse oximeter and assessing the pink color of the mucosa.
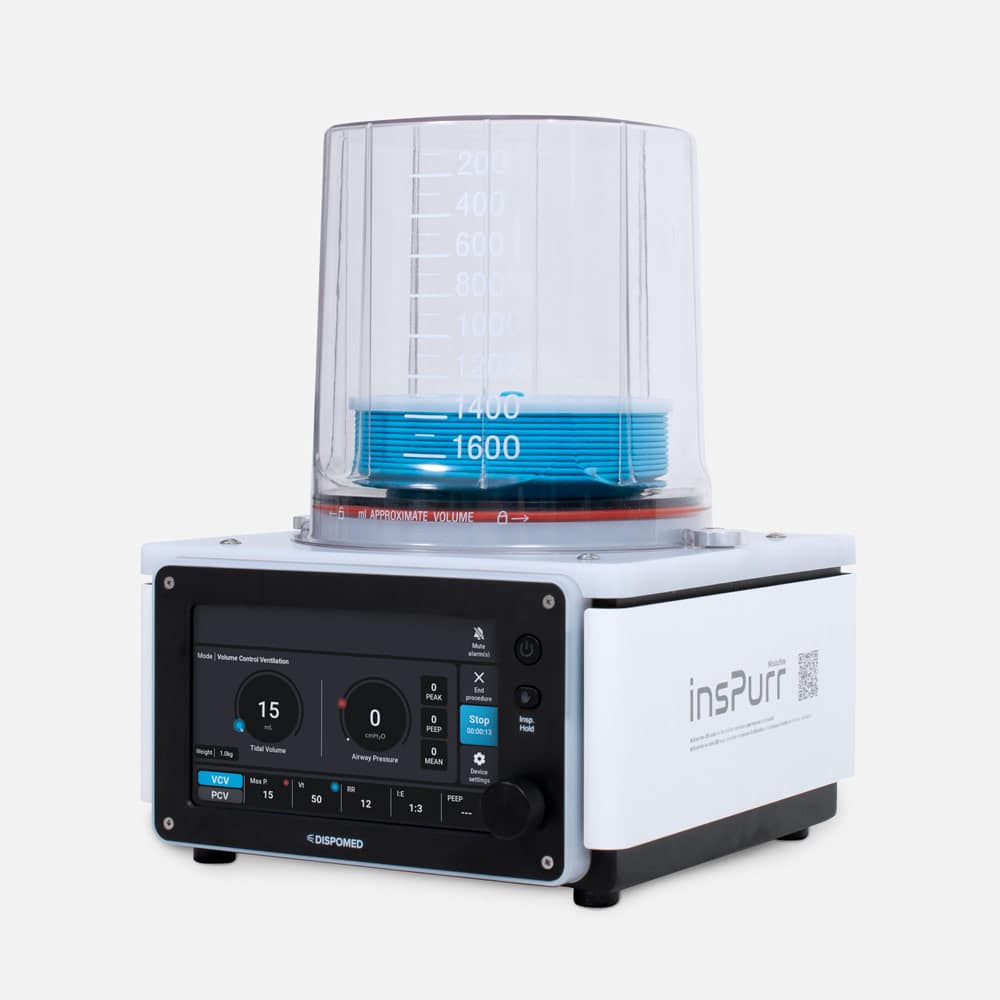
When choosing a mechanical ventilator, many options feature a bellows-style construction that can be powered pneumatically or by a piston or turbine. Some models also incorporate microprocessors to assist with operation. Pneumatic-driven ventilators tend to have high oxygen consumption.
Key features to look for include safety pressure alarms and relief valves. It’s essential to have an anesthesia machine pressure alarm in place when a ventilator is in use to avoid accidental closure of the pop-off valve. Additionally, some pop-off valves come with specialized safety features that prevent users from closing the valve while the ventilator is active. Pressure occlusion typically occurs when a cap is in place.
Newer ventilators, such as the Inspurr, utilize turbine-driven technology, consuming zero liters of oxygen per minute to operate the bellows. These models are quieter and considered safer, thanks to their internal respirometry that measures the patient’s lung volume, ensuring accurate positive pressure delivery.
References:
Cooley, Kristen G. & Johnson, Rebecca A. (2018). Veterinary Anesthetic and Monitoring Equipment. Hoboken: Wiley and Sons
Dorsch & Dorsch, 5th ED (2007). Understanding Anesthesia Equipment. Baltimore: Lippincott Williams & Wilkins
Seymour, Chris & Duke-Novakovski, Tanya. (2016). BSAVA Canine and Feline Anaesthesia and Analgesia, 3rd ED. Gloucester: BSAVA


Veterinary Specialist Articles